What is epilepsy?
Epilepsy is a combination of diverse chronic neurological disorders, which is usually characterized by unpredictable and unprovoked recurrent seizures. The disease is caused by eternal alteration in brain tissue, which results in over impulsive brain. The overexcited brain thus conveys abnormal signals, which in turn causes repeated and unpredictable seizures. However, a single seizure that does not repeat again is not considered as epilepsy. Although,in some cases of epilepsy, a single seizure in combination with brain alteration can increase the likelihood of future seizures.The disease affect a variety of mental and physical functions such assensory, motor, and autonomic function; consciousness; emotional state; memory; cognition or behavior. Epilepsy is represented as one of the most common neurological diseases that affect about 50 million of people worldwide. The onset of epileptic seizure is manifested by unusual, excessive and hypersynchronous discharge of neurons in the over excited brain.The cause of epileptic seizure may be genetic background or the severe brain injury or family propensity towards the disease.However the exact cause of epilepsy largely remains unknown. Some of the possible common causes of epilepsy include stroke, Alzheimer’s disease, trauma, brain injury, congenital birth defect, metabolism disorder, brain tumor, brain infection (e.g. meningitis, encephalitis and brain abscess) and medication (amphetamines cocaine, tramadol, and antidepressants). The onset of epileptic seizure typically begins at the age between 5 to 20, but not strictly adheres to this age group and can happen at any age.The symptoms of epilepsy may vary from patient to patient and comprise from simple staring spells to violent shaking and loss of consciousness. The Physical examination such as electroencephalogram (EEG) and Head CT or MRI can be performed to check the abnormal electrical activity and its accurate location in the brain. The treatment of epilepsy is principally based on seizure preventing medications. However, in case of unsuccessful medication, other therapy such as surgery, complementary therapy, or vagus nerve stimulation, changes in diet or special diet are also tried.
Is epilepsy and seizures the same thing?
The term epilepsy and seizure closely resembles each other and therefore erroneously interchanged. However, in spite of the close association between the epilepsy and seizure, they should not be considered the identical or same clause. In this respect, a precise distinction and delineation between seizures and epilepsy is highly essential. A seizure is medically described as a brain dysfunction that results in altered attention or behavior. Seizures are mainly caused due to episodes of disturbed brain activity, which result in unnecessary hypersynchronous discharge of a population of cortical neurons. A seizure can beoften encountered under the condition of brain injuries or chemical imbalances, or infections which can irritate the brain. Whereas Epilepsy is marked as a disorder of the central nervous system in which a person has multiple or repeated seizures over time. Therefore, a person with epilepsy has seizures, but seizure patient don’t necessarily has epilepsy. The precise distinction between epilepsy and seizures is essential to focus the diagnostic approach and to select the appropriate drug therapy. Since, in case of epilepsy chronic treatment, such as antiepileptic medication or surgery might be required, whereas for an isolated seizure the common therapy is directed towards the underlying cause and not towards antiepileptic drugs (AEDs). The concepts of seizures and epilepsy become more obvious in view of the basic anatomic and electrophysiologic properties of the cerebral cortex. The major criteria of clear delineation comprise the factors that determine the level of neural activity at the cellular and cell network level and electroencephalogram (EEG). Clinical studies suggested several kinds of seizures, which areattributed with specific behavioural changes and electrophysiological disturbances and detected by electroencephalographic (EEG) recordings. Doctors recommend that a single seizure does not essentially signify that a person has epilepsy. According to them, approximately 10 percent of adults experience a seizure at some point in their lifetime, but the two-third of them will never experience it again.The characteristic symptoms of epileptic seizures include a loss or change of alertness, jerking and ripple movements of the arms or legs, difficulty in speaking and lip-smacking. Non-epileptic seizures, or pseudo-seizures or psychogenic seizures, also closely resemble with epilepsy thus making diagnosis difficult.
Connection between Autism and epilepsy
Epilepsy and autism represent a group of heterogeneous clinical disorders associated with behaviorally defined, neurodevelopmental disorders. Seizures are relatively common and most prevalent neurological disorder associated with epilepsy and autism or autistic spectrum disorder. It has been observed that epilepsy is frequently developed in individuals with autism or autistic spectrum disorders (ASD). Prevalence studies suggested that seizures in autistic patients develop either in childhood or at puberty or adulthood. However, the risk of seizure particularly remains high at adulthood in autistic patients. Clinical data estimated that the frequency of epilepsy is comparatively larger than the prevalence of active epilepsy in the general population. Studies on autistic patients has established that as many as ~ one third of children with autism also have epilepsy. This risk is comparatively higher in autistic patients with severe mental retardation, genetic abnormalities and brain malformations. It has been proposed that abnormalities in brain of autistic patients can disrupt the cortical neuron and therefore alter brain activity. Overload or disturbances in brain neurons result in unusual, excessive hypersynchronous electrical discharge of a population of cortical neurons, thus contribute to increased risk of seizure. Clinical studies suggest that during epilepsy regression of language, behaviour and cognition further develops the clinical manifestations that resemble with the behavioral syndrome of autism. The common risk factors which increased the probability of coexistence of both epilepsy and autism comprisegenetic factors, language impairment, severe cognitive dysfunction, motor deficits, symptomatic etiology, and onset of seizure.
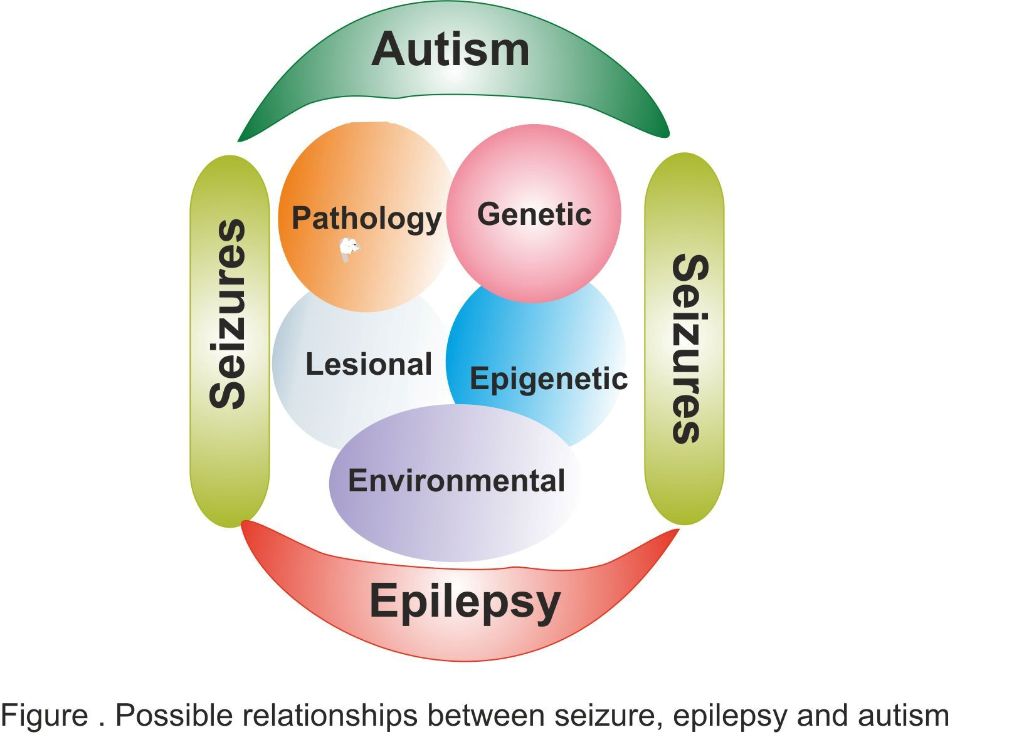
Clinical studies suggested a possible association between epilepsy and autism. Recent studies suggested the sharing of common predisposing genes between epileptic and autistic individuals. Studies conducted by Patrick Cossette and research team reported that nonsense andmissense mutations in synapsin gene (SYN1) were associated with ASDs, epilepsy, or both. Cossette and co-workers observed that these mutations were associated with functional defects in nerve terminal function. The synapsin 1 is the member of synapsin family of neuronal phosphoproteins, which are associated with the synaptic vesicles present in the central and peripheral nervous systems.This family of proteins are implicated in synaptogenesis and in modulation of neurotransmitter release, thereby playing a potential role in neuropsychiatric diseases.More recently, in year 2012, studies conducted by Joseph G. Gleeson and team suggested the possible involvement of another gene BCKDK (Branched Chain Ketoacid Dehydrogenase Kinase) in consanguineous families with intellectual disability such as autism and epilepsy. The research team has identified inactivating mutations in the gene BCKDK in autistic and epileptic patients. The protein encoded by BCKDK (Branched Chain Ketoacid Dehydrogenase Kinase) is accountable for phosphorylation-mediated inactivation of the E1α subunit of branched-chain ketoacid dehydrogenase. It has been observed that BCKDK knock-out mice display abnormal amino acid profile in brain and neurobehavioral shortfalls.Apart from this, the likelihood of interaction among the pathophysiology of neural circuits could lead to autistic or conversely could predispose the brain to seizures. However, the possibilities are not mutually exclusive and the underlying mechanisms responsible for increased seizure susceptibility in autistic individual are not yet clear. The clinical and neurobiological aspects as well as the mechanisms answerable for cellular hyperexcitability in autism and epilepsy are likely to involve the interplay of genetic, epigenetic, and environmental factors. It has been postulated that the possible relationships between brain development, epilepsy and ASD might be a common neurobiological antecedent. This includes genetic susceptibilities or structural or developmental abnormalities or environmental insults, which possibly lead to abnormal brain development. The varied etiologies of autism and epilepsy make it improbable that single universal machinery can explain seizure tendency in both disorders.In view of this, future studies point to potential genetic links of neural circuits and cellular signaling pathways directed to neural hyperexcitability in epilepsy and autism and need to be reviewed in detail.
Suggested References
Epilepsy: Medical Encyclopedia. Pubmed health
Berg, A. T. and S. Plioplys (2012). “Epilepsy and autism: is there a special relationship?” Epilepsy Behav 23(3): 193-198. Abstract
Thompson, A. W., R. Kobau, et al. (2012). “Epilepsy care and mental health care for people with epilepsy: California Health Interview Survey, 2005.” Prev Chronic Dis 9: E60.Abstract
Stafstrom, C. E., P. J. Hagerman, et al. (2012). “Pathophysiology of Epilepsy in Autism Spectrum Disorders.”Abstract
Novarino, G., P. El-Fishawy, et al. (2012). “Mutations in BCKD-kinase lead to a potentially treatable form of autism with epilepsy.” Science 338(6105): 394-397.Abstract
Berg, A. T., S. Plioplys, et al. (2011). “Risk and correlates of autism spectrum disorder in children with epilepsy: a community-based study.” J Child Neurol 26(5): 540-547.Abstract
Theoharides, T. C. and B. Zhang (2011). “Neuro-inflammation, blood-brain barrier, seizures and autism.” J Neuroinflammation 8: 168.Abstract
Fassio, A., L. Patry, et al. (2011). “SYN1 loss-of-function mutations in autism and partial epilepsy cause impaired synaptic function.” Hum Mol Genet 20(12): 2297-2307.Abstract
Levisohn, P. M. (2007). “The autism-epilepsy connection.” Epilepsia 48 Suppl 9: 33-35.Abstract
Tuchman, R. (2006). “Autism and epilepsy: what has regression got to do with it?” Epilepsy Curr 6(4): 107-111. Abstract
Fisher, R. S., W. van Emde Boas, et al. (2005). “Epileptic seizures and epilepsy: definitions proposed by the International League Against Epilepsy (ILAE) and the International Bureau for Epilepsy (IBE).” Epilepsia 46(4): 470-472.Abstract
Suggested Articles:
1. Autism and Vaccines
2. Autism and Depression
3. Autism and Bad Behavior
4. Autism and Schizophrenia
5. Autism and Alzheimer’s
6. Autism and Crohn’s disease
7. Autism and Dyslexia
Is it just me or does it appear like a few of these responses appear like they are written by brain dead individuals? 😛 And, if you are writing at additional sites, I would like to follow everything fresh you have to post.Would you make a list of the complete urls of your social community pages like your Facebook page, twitter feed, or linkedin profile?
Excellent goods from you, man. I have remember your stuff previous to and you’re just too magnificent.
I really like what you’ve bought here, really like what you’re stating and the way in which through which you say it.
You are making it entertaining and you continue to care for to keep it sensible. I cant wait to learn far more from you. This is actually a tremendous site.